



What is Blood Flow Restriction Training?
The Physiological Responses to Blood Flow Restriction Training in Regard to Strength Training and Physical Therapy
THE DREAM
Building more muscle in a shorter timeframe with less effort and decreased injury.
THE GIST
With Blood Flow Restriction Training (BFRT), a cuff or a tourniquet is applied to the athlete or patient’s proximal limb in order to limit blood flow into and out of the working muscle. During normal strength training, a person needs to lift at least 70% of their one repetition maximum (aka High Intensity Training) to increase strength and hypertrophy. The addition of BFR during exercise requires that the patient lift only 20-40% of their one repetition maximum (aka Low Intensity Training) to see strength and hypertrophy gains.
THE SCIENCE
Hypoxia
When we go from resting to exercising there is an increase in blood flow. With BFRT we want to restrict just enough blood flow to allow the limb to become hypoxic while also avoiding complete occlusion. Hypoxia is a decrease of oxygen in the muscle. At first glance, this sounds like it would be detrimental to the muscle but if we take a closer look at our body’s energy systems, we can conclude this results in increased muscle size and strength.

Energy Systems
Our bodies require energy for our training sessions and there are two energy systems that we could utilize during exercise depending on the intensity of the workout.
1. Aerobic Respiration – requires oxygen to produce energy
2. Anaerobic Respiration – does not require oxygen to produce energy
Aerobic Respiration
The higher the intensity of exercise the shorter amount of time it can be sustained. The same is true for the opposite; the lower the intensity of exercise the longer amount of time it can be sustained. Aerobic Respiration is the process by which we use oxygen to turn fuel (the food we eat) into energy. Oxygen use will kick in after about 2 minutes of exercise, so low intensity resistance training will utilize the aerobic energy system. This is because we only need to utilize our smaller motor units when the intensity is low. In short, slow twitch fibers do not produce enough muscle contraction to help with strength gain.
Size Principal
The other thing to note about our muscle fibers is that they follow the Size Principal, or Sequential Recruitment. This means that when we start an activity or exercise, our body uses the lowest energy, or the smallest muscle fibers first. If they are not sufficient enough to complete the task, the next level of fibers are recruited and so on, up to the larger, high energy fast-twitch fibers. When we start recruiting these fast twitch fibers the energy needed is more substantial so our bodies transition into utilizing lactate as energy. Enter: Aerobic Respiration.
Anaerobic Respiration
The energy system that produces the most muscle gain is the anaerobic energy system. This is because without the use of oxygen for energy production, our bodies are forced to produce lactate, which is metabolized as energy. In fact, our bodies actually prefer lactate as a fuel source and our muscles will contract stronger with lactate. When using lactate as an energy source, our bodies must recruit the largest motor units in order to overcome fatiguing too quickly. The larger motor units will fire our fast twitch muscle fibers, which have been shown to be essential for strength and hypertrophy change.
However, when you add BFR training to low intensity resistance training, the body is tricked into using the anaerobic system instead due to the decrease of oxygen in the muscle. Using BFR, you can exercise using significantly less weight and still achieve substantial gains in muscle strength and size.
Cellular Swelling and Muscle Protein Synthesis
In order for BFR to be effective, the cuff must be tight enough to restrict the veins in the arms or legs from returning blood from the muscles to the heart, but not so tight that it stops fresh blood traveling from the heart to the muscles. Blood is able to enter the muscle via arterial flow; however, the veins are restricted so that blood is partially prevented from leaving the working muscle. This creates a buildup of blood in the muscle, which leads to cellular swelling. The body perceives this sudden swelling as a threat to the structure of the cell and its survival. In order to combat this threat, the cell will trigger Muscle Protein Synthesis. Muscle Protein Synthesis (MPS) is the process by which protein is produced in order to repair muscle damage after a workout. When the muscles go through this repairing process, they are also adapting to the stresses put on them, so they end up repairing themselves to be bigger and stronger than they were before in order to prepare for the next training session.
Muscle Protein Breakdown
The main reason to use BFR is that we can lift light loads but adapt like high loads. Research shows that High Intensity Training (HIT) and Blood Flow Restriction with Low Intensity Training (LIT) will result in comparable strength and muscular size gains due to similar increase in fiber recruitment. However, HIT will also result in increased muscle damage while BFRT shows no increase in muscle damage. Muscle damage can also be referred to as Muscle Protein Breakdown. Muscle Protein Breakdown (MPB) is the loss of protein during a workout. In normal HIT training, MPB is needed in order to trigger MPS. Because of MPS and MPB, our bodies are in a constant state of protein turnover, which is an important component of muscular adaptation and remodeling in strength training when a BFR cuff is not involved. However, with no significant muscle damage during BFRT and protein synthesis already being triggered by cellular swelling, there is very little recovery time required. Because of this, our body doesn’t need to go through the process of repairing damage before seeing strength gains, it is able to immediately adapt.
THE APPLICATION
In a Physical Therapy setting we are typically seeing patients who already have some sort of damage, likely an injury to soft tissue or boney structures. With any injury, we tend to see atrophy in surrounding musculature. BFRT has been shown to decrease post-injury or post-surgery atrophy while avoiding any unnecessary strain in injury or surgical site. After most injuries, especially surgeries, there is a period of time that we must respect the tissue healing timelines as well as pain level of the patient by utilizing lower loads. These lower load exercises are not heavy enough to induce a hypertrophic or strength stimulus to the exercising muscle, unless we add BFR to the mix.

THE SAFETY
History
Even though you may have just started to hear more about BFRT, it has actually been safely utilized in Japan for around 50 years. The United States has been utilizing BFRT since 2014 and it has been formally recognized within the scope of practice for Physical Therapists since 2018.
Limb Occlusion Pressure
To make sure that BFRT is being safely implemented, there are specific parameters the Physical Therapist must follow. For each individual patient, Limb Occlusion Pressure (LOP) must be determined. This is the minimum amount of pressure needed to occlude blood flow to and from the limb. It is important to note that with BFR we are intending to restrict the arterial blood flow, not actually occlude it. Full occlusion of arterial blood flow to an extremity could lead to many complications. Instead, the PT will find the limb occlusion pressure using a doppler ultrasound and then take a percentage of that occlusion pressure for the patient to work under. The percentage will likely fall between 40 and 80 percent depending on intended benefit.
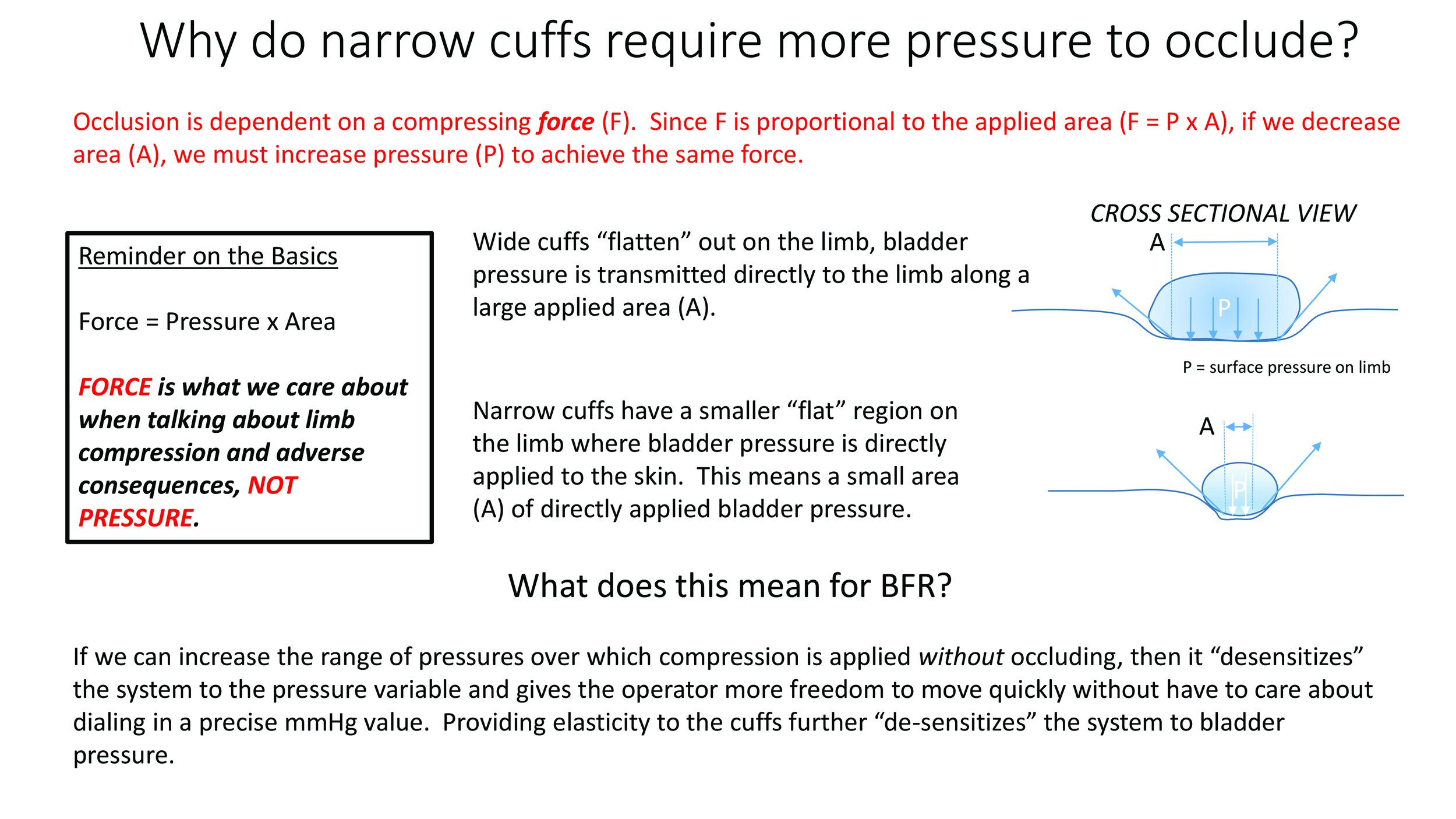
Cuff Width
The other thing the PT will consider is the width of the cuff. It is recommended to use a cuff that is wide, as you will need less pressure to restrict arterial inflow. A wider surface area means lower pressure distributed below the cuff, which is potentially safer for the more delicate nerves and blood vessels that are also below the skin.
Contraindications
The last thing to consider before utilizing BFRT on a patient is determining any contraindications involved. Contraindications for BFR include history of deep-vein thrombosis, pregnancy, varicose veins, high blood pressure, cardiac disease and rhabdomyolysis.
THE REALITY
Effectively implementing BFR in combination with LIT will in fact build more muscle in a shorter timeframe with less effort and decreased injury.