


What Is Little League Shoulder?
Chances are that you have heard the term Little League Shoulder. Most have encountered it in the media, during youth playing days, or from their own children. This article was written to provide some clarity about youth shoulder pain.
Little League shoulder is an injury to the growth plate in the upper arm. It occurs at the “ball” of the “ball and socket” that forms your shoulder and includes various stages of pathology:
Apophysitis:
Irritation and inflammation (without fracturing) of the growth plate.
Avulsion fracture/separation:
Fracturing and separation of the growth plate from the rest of the bone in your upper arm.
Little League shoulder, also known as proximal humeral epiphysitis, is a common overuse injury that affects young baseball players, typically between the ages of 8 and 15. It is characterized by pain and discomfort in the shoulder joint, specifically in the upper arm bone (humerus) near the growth plate.
The condition occurs due to repetitive stress and excessive strain placed on the developing shoulder joint during activities like pitching, throwing, and overhead motions.
Shoulder Anatomy Review: The Basics
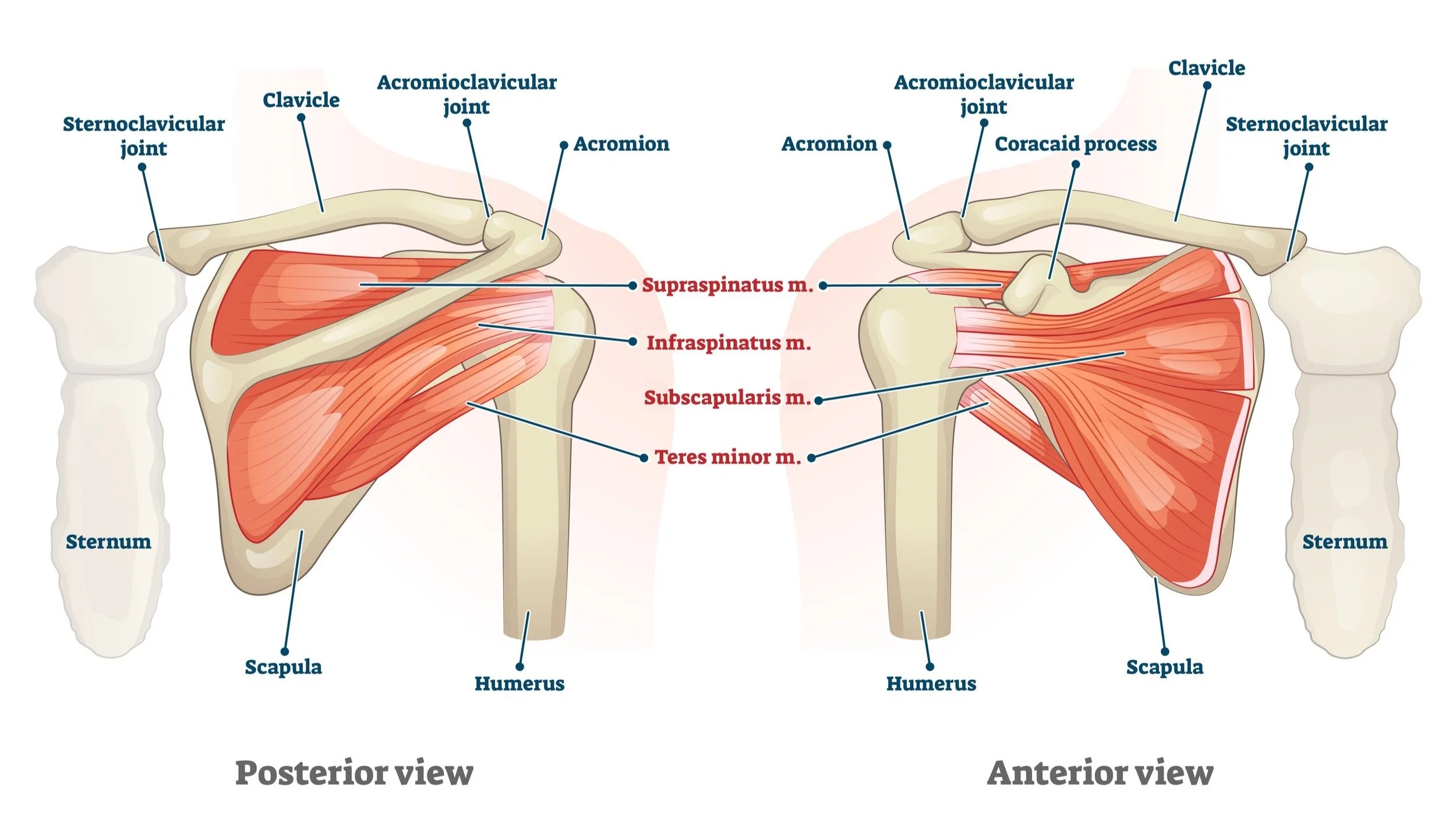
The anatomy described below is involved in Little League shoulder.
Bones:
Humerus
Also known as the upper arm bone. The top of this bone forms the “ball” of the “ball and socket” shoulder joint. The growth plate, which is medically known as an apophysis that is injured in Little League shoulder is located here.
Scapula
Also known as the shoulder blade. This bone forms the “socket” of the “ball and socket” shoulder joint and attaches to the rib cage.
Muscles:
Rotator cuff
The collective group of muscles in charge of keeping the ball and socket together during movement, such as throwing.
Back/Scapular muscles
The collective group of muscles located on the back, in charge of controlling the shoulder blade itself. This includes the rhomboids, traps, lats, and serratus anterior.

What Causes Little League Shoulder?
Little League shoulder is primarily caused by excessive throwing volume, throwing intensity, and poor workload management. It is an overuse injury that usually occurs between the ages of 8 and 15. It is caused by several factors leading to excessive stress levels in the growth plate of the upper arm. Little League shoulder is primarily caused by the combination of skeletal immaturity and high-intensity throwing, which can lead to stress and microfractures in the growth plate area.
Amount of Throws A Pitcher Makes Per Week
How much an athlete is throwing plays the largest single role in the development of Little League shoulder. For information on how much stress is placed on an athlete’s shoulder, see:
Regular Season Pitching Rules - Little League
Pitch Smart | Guidelines | MLB.com
When an athlete is starting the season or has not been throwing for a while, they will need to perform a gradual, progressive return to throwing. This allows the athlete’s body to slowly adapt to the stressors placed on the arm during sport.
““It is critical for the athlete have honest communication with the coach as this is the greatest prevention of season ending injuries.””

The Intensity of Pitching and it’s Impact
Not all throws are created equal. Playing light catch in the backyard is much different than max intensity pitching. Higher intensity throwing places greater levels of stress on the athlete’s body and, therefore, increases the strain placed on the shoulder growth plate.
Do Throwing Mechanics Matter?
Poor throwing mechanics can lead to excessive stress levels on the athlete’s shoulder/arm. This may increase the strain on the growth plate and can play a role in the development of Little League shoulder.
Studies also show that throwing hard in and of itself increases arm stress/torque. Therefore, the harder a kid throws and the better the kid gets at baseball, the more stress he will create in his shoulder. It is not uncommon to see the player with the best mechanics, who also throws the hardest, develop Little League shoulder—especially if this player is used most often for pitching and playing shortstop or other positions with high throwing demands.
Throwing of any kind causes stress to the shoulder. This is true regardless of whether the athlete has the best or worst mechanics and is the reason focus should be applied to workload management when trying to prevent Little League shoulder.
““Too much stress can lead to injury, stress is a product of power and power is necessary for progression in baseball”.
”

Does Pitch Type Matter in Relation to Injury?
It has long been believed that throwing curveballs from a young age can cause Little League shoulder. This is not the case. Throwing too much of any pitch type can cause growth plate irritation. In fact, many recent studies have shown that fastballs create greater stress levels on the arm than curveballs.
How Do You Treat Little League Shoulder?
Little League shoulder is primarily treated with rest and reduced throwing volume. The athlete must reduce aggravating factors and allow for the bone to heal.
If no fracturing or excessive separation of the growth plate has occurred, the athlete can sometimes continue playing baseball with modified activity and reduced volume/intensity of throwing.
If clear and significant growth plate separation or fracturing has occurred, the athlete must stop throwing entirely (usually for a minimum of 4 to 6 weeks).
Physical therapy is recommended to help improve mechanics, increase strength, and reduce the stress being placed on the growth plate once the athlete returns. A gradual return-to-throw program will also need to be implemented to help the athlete ramp up throwing activities safely. I highly recommend seeking a baseball specialist physical therapist to ensure sport-specific rehabilitation, as well as proper return to throwing.
How Do You Prevent Little League Shoulder?
No one can guarantee the prevention of Little League shoulder. There are ways, however, to lessen the chance of developing it.
Practice proper arm care, including warming up and cooling down.
The warm-up should increase the athlete’s heart rate, get blood flowing, and cause a light sweat. It should include movements that work the rotator cuff and shoulder blade but do not completely fatigue these muscles. The cool-down should be similar to the warm-up and should work the athlete’s throwing arm to help promote fluid return and muscle activation. The cool-down should not consist of wrapping the arm in ice and sitting still.
Manage the workload and monitor throwing amounts.
The single best way to prevent Little League shoulder is to avoid overuse and over-throwing. Workload management is a complex equation involving the volume of throws, the intensity of throws, and the frequency with which they are performed. For more information on how to avoid excessive workload amounts, speak with your coach, a medical professional or review the guidelines online.
““Shoulder pain or even slow developing pain is something that should be looked at by a physical therapist or shoulder specialist.””

DON'T THROW THROUGH PAIN!
Throwing is a violent motion that puts extreme amounts of strain on the athlete's arm. Don’t freak out if little Johnny has one or two days of pain after a long outing. This is common. However, don’t have little Johnny push through pain or throw with continued pain for long periods of time. I recommend seeing a medical provider, such as a baseball-specific physical therapist, if throwing pain persists for 1-2 weeks or longer.
The Bottom Line
Little League shoulder is an injury to the growth plate in the upper arm. It usually refers to the separation of the growth plate from the rest of the bone.
Little League shoulder is caused by many factors, primarily excessive throwing volume and intensity.
Little League shoulder is treated with rest and a reduction in throwing.
Physical therapy and sport modification are also crucial for the treatment of Little League shoulder.
About the Author:
Jordan Bork (PT, DPT, CSCS, CFSC) is an orthopedic and sport physical therapist who specializes in overhead athletes and baseball/softball rehabilitation. He works full-time at LWPT Kirkland and part-time at Driveline Baseball in Kent. Jordan treats patients of all competitive levels, including professional and college; however, his passion is in youth athletics ranging from Little League to high school.
AUTHOR:
Jordan Bork, PT
Physical Therapist and Baseball Specialist
CONTRIBUTORS:
Terry Phillips, PT, DPT
Physical Therapist and Baseball Specialist
Joe Midgett, PT, DPT
Physical Therapist and Baseball Specialist
Bob Adams, DO
Sports Medicine Physician and Former head of the medical team for USATF
Avi Goodman, MD
Evergreen Health Orthopedics & Sports Medicine
Samuel Koo, MD
Orthopedic Surgeon, ProOrtho
Vincent Santoro, MD (Retired)
Orthopedic Surgeon and former college pitcher
Ben Wobker, PT, MSPT, CSCS, CFSC, SFMA
Founder & Director LWPT
MORE BLOGS


MORE WEBINARS
REFERENCES
Chandra, Venita, et al. “Thoracic Outlet Syndrome in High-Performance Athletes.” Journal of Vascular Surgery, vol. 58, no. 2, 2013, pp. 567–568., doi:10.1016/j.jvs.2013.05.086.
Ferrante, Mark A., and Nicole D. Ferrante. “The Thoracic Outlet Syndromes: Part 2. The Arterial, Venous, Neurovascular, and Disputed Thoracic Outlet Syndromes.” Muscle & Nerve, vol. 56, no. 4, 2017, pp. 663–673., doi:10.1002/mus.25535
Hangge, Patrick, et al. “Paget-Schroetter Syndrome: Treatment of Venous Thrombosis and Outcomes.” Cardiovascular Diagnosis and Therapy, vol. 7, no. S3, 2017, doi:10.21037/cdt.2017.08.15.
Otoshi, Kenichi, et al. “The Prevalence and Characteristics of Thoracic Outlet Syndrome in High School Baseball Players.” Health, vol. 09, no. 08, 2017, pp. 1223–1234., doi:10.4236/health.2017.98088.
Sanders, Richard J, et al. “Diagnosis of Thoracic Outlet Syndrome.” Journal Of Vascular Surgery, vol. 46, no. 3, Sept. 2007, pp. 601–604., www.sciencedirect.com/science/article/pii/S0741521407007343.
Thompson, Robert W. “Thoracic Outlet Syndrome and Neurovascular Conditions Of The Shoulder In Baseball Players.” Baseball Sports Medicine, by Christopher S. Ahmad and Anthony A. Romeo, Wolters Kluwer, 2019.
Watson, L.a., et al. “Thoracic Outlet Syndrome Part 1: Clinical Manifestations, Differentiation and Treatment Pathways.” Manual Therapy, vol. 14, no. 6, 2009, pp. 586–595., doi:10.1016/j.math.2009.08.007.
Watson, L.a., et al. “Thoracic Outlet Syndrome Part 2: Conservative Management of Thoracic Outlet.” Manual Therapy, vol. 15, no. 4, 2010, pp. 305–314., doi:10.1016/j.math.2010.03.002.
Popkin, C. A., Bayomy, A. F., & Ahmad, C. S. (2019). Early Sport Specialization. Journal of the American Academy of Orthopaedic Surgeons, 27(22), e995–e1000.
DiFiori JP, Benjamin HJ, Brenner JS, et al. (2014) Overuse injuries and burnout in youth sports: a position statement from the American Medical Society for Sports Medicine. British Journal of Sports Medicine; 48:287-288.
Post EG, Trigsted SM, Riekena JW, Hetzel S, McGuine TA, Brooks MA, Bell DR. (2017). The Association of Sport Specialization and Training Volume with Injury History in Youth Athletes. Am J Sports Med; 45(6):1405-1412. doi: 10.1177/0363546517690848.
Buckley PS, Bishop M, Kane P, Ciccotti MC, Selverian S, Exume D, Emper W, Freedman KB, Hammoud S, Cohen SB, Ciccotti MG. (2017). Early Single-Sport Specialization: A Survey of 3090 High School, Collegiate, and Professional Athletes. Orthop J Sports Med. 28;5(7)
Bell DR, Post EG, Biese K, Bay C, Valovich McLeod T. (2018). Sport Specialization and Risk of Overuse Injuries: A Systematic Review With Meta-analysis. American Academy of Pediatrics; 142(3)
Myer, G. D., Jayanthi, N., DiFiori, J. P., Faigenbaum, A. D., Kiefer, A. W., Logerstedt, D., & Micheli, L. J. (2016). Sports Specialization, Part II: Alternative Solutions to Early Sport Specialization in Youth Athletes. Sports health, 8(1), 65–73.
Disclaimer: The information listed on this page is not to be used as medical advice. If you have any questions or concerns regarding stretching, mobility, or strength training, please seek out professional attention.