


Fundamentals of Bone Stress Injuries
What is a bone stress injury (BSI) and how do I know I have one? How long will it take to get me back to running? As a physical therapist who treats a lot of runners and as a lifelong runner myself, I have always had a passion for keeping runners running. The act of running can make someone’s day tick along better, can help with consistent sleep, calm the nerves and can even make a runner more fun to be around. It can be social or an act of solitude. It can be alarming for a runner when they start to experience a nagging pain that doesn’t warm up or even worsens as they run. Pain that doesn’t dissipate with a warm-up routine or is vague at first but then becomes localized or intensifies through the run can be a sign of a bone stress injury or BSI. BSI is a general term indicating mechanical load is exceeding the bone’s structural ability to withstand the load. However, BSIs occur on a continuum. One end of that continuum is a stress reaction, the other end can be stress fracture or even a full fracture of the bone. The runner recognizes this as pain that isn’t normally present. BSIs can occur for many reasons whether due to biomechanics or from a nutritional standpoint or a combination of both. As high-school and college cross-country runners prepare now for this upcoming season, they should be aware of the common causes and ways to prevent bone stress injuries.

I recently completed a 6-week Stress Fracture School with PT, Nathan Carlson, who works with recreational and elite runners including USTAF athletes (1). You may recognize him from his guide to return to running after a stress fracture injury. Combat Stress Fractures | RunningMateKC He is based in Kansas City but I had the opportunity to listen in via Zoom with 33 other physical therapists across the country, where we reviewed research articles, shared cases and generally discussed how to work with runners as their bone stress injuries heal. I wanted to cover some of the topics we discussed as well as share insights from one of my mentors, Dr. Bob Adams, who served as the chair of USTAF Sports Medicine and Science Committee and was team physician for multiple World Championships and Olympic Teams. To complete the list of heavy hitters, I interviewed Dr. Kelly Pritchett, Director of the Nutrition Graduate Program at Central Washington University and Board Certified Specialist in Sports Dietetics. You may recognize her from her article in Runner’s World titled “What Runners Need to Know about Ferritin Levels and Iron Deficiency”.
Diagnosis of a Bone Stress Injury
Diagnosis of a BSI injury can sometimes be delayed if runners don’t recognize the signs and symptoms. Dr. Adams stresses that a lot of elite athletes have access to the most current sound advice but can still develop these injuries. He notes it is important to consider that it takes time to gain bone back after a period of immobilization whether due to injury or lack of activity. He adds that time spent on your feet at a summer job and factors like weight loss, tobacco use and alcohol use or not having enough time between sports seasons are all factors that should be considered. According to Dr. Adams, “The most important part of training is recovery and the most important part of recovery is sleep”. (2) He adds that when runners run slower than they would like to or feel their performance is poor they may sometimes use that as a cue to run more. This can lead to symptoms of overtraining. Dr. Adams says, “Bone health depends upon many interrelated factors including genetics, nutrition, bone load and adequate recovery. Early recognition and intervention is imperative.” (2)
““Bone health depends upon many interrelated factors including genetics, nutrition, bone load and adequate recovery. Early recognition and intervention is imperative.” ”
Fortunately, we can utilize new state of the art research on nutrition, biomechanics and coaching techniques. According to Dr. Pritchett, “Under-fueling can lead to low energy availability (LEA) which has negative physiological, health, and performance consequences. LEA occurs when energy intake is insufficient to support normal physiological function after energy is expended for exercise. LEA can be the result of disordered eating but can also be unintentional due to a lack of knowledge about fueling needs”. (3) Along with smart training plans and paying attention to an algorithm of nutritional factors, endocrine function, metabolic function and hormone function, BSIs can be treated appropriately or avoided altogether. For many runners, we increase our volume of running as we seek to keep challenging ourselves with new distances or faster times but we don’t always match that increase with proper nutritional guidelines for runners (which can be different than non-runners). Whether someone is a casual runner or competitive racer, it’s important to set yourself up for successful bone health. That might mean a gait analysis by a PT trained in treating runners and/or a consult with a registered sports dietician. The physician is responsible for ordering blood tests and diagnostics like X-ray and MRI and directs the care plan so an individual doesn’t run too much too soon.
What is Relative Energy Deficiency in Sport

Connor Inslee resting his eyes after a long day on the trail. Photo Credit: Nick Spang
You may have come across the term RED-S in your running magazines, social media or favorite blog. RED-S means Relative Energy Deficiency in Sport. It has replaced the term Female Athlete Triad (disordered eating/low energy availability, menstrual dysfunction and decreased bone mineral density). This change was made as it was determined that males can also have these issues and there are other issues that contribute to RED-S including metabolic, gastrointestinal and growth and development factors. (3,4) It can be common in what Nathan calls “leanness sports”, like distance running when people sometimes get in the habit of eating less than their body needs. You can see the difference in body types of endurance runners versus sprinters in the Olympics. One athlete type tends to be leaner than the other. Depending on the goals of a runner, it might feel like you are lighter on your feet and therefore run faster when you are essentially limiting your calories. However, even short periods of low energy availability (ie 5 days) can alter bone metabolism (5). So it’s important to think of energy availability just as you think about how many miles you are going to run that day. Otherwise, a runner may be at an unintentional risk for RED-S. RED-S can lead to osteopenia or osteoporosis which are risk factors for bone stress injury.


Bone Adaption Considerations
According to Nathan, bones like odd and unpredictable impact (ie soccer, basketball and volleyball). It’s important to use sensible training plans. For example, when it’s your off-season for running/racing try to expose yourself to varied types of exercise. Include strength training for runners. Consult a PT experienced with working with runners for an individual evaluation of your needs and get a detailed list of the best exercises for you. If you find you have had repeated stress fractures or they take a long time to heal, consider working with a registered dietician (RD). Dr. Pritchett explains, “Ensure vitamin D levels are adequate to support bone health and to help with calcium absorption. Depending on vitamin D levels, supplementation may be needed (especially during the winter months) to ensure levels are >50 nmol/L. Although sunlight is the best source of vitamin D, dietary sources include fatty fish, sun-exposed mushrooms, sardines, and milk”. (3)
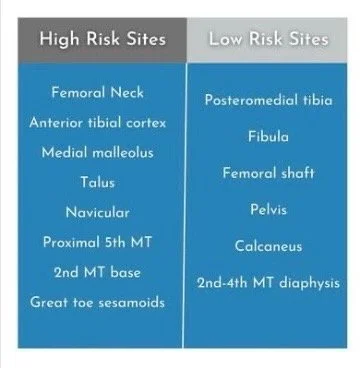
Bones assist in movement and muscle contraction. You can think of our bodies as a series of pulleys and levers. They also help produce red blood cells. We even have different types of bone: cortical bone on the edges of the long bones and cancellous or spongy bone at the end of the long bones. How bone responds to load is site-specific. Not all stress fractures are alike as there are low-risk sites and high-risk sites. These are determined by the type of load. Low-risk sites are on the compressive side of the bone (squeezing forces). High-risk sites are on the tensile side of the bone and often don’t have as much of a blood supply. Low-risk sites include the tibial shaft, fibula, calcaneus and metatarsal shaft amongst others. High-risk sites include the femoral neck, anterior tibia (anterior cortex), proximal 5th metatarsal, sesamoid of the big toe, talus and navicular amongst others. Low-risk sites tend to take up to 8 weeks to heal. High risk sites can take up to 22 weeks to heal. (1) Dr. Adams stresses that these healing time frames are good ballpark figures but it can take longer for healing to occur. (2) In one study (6), subjects showed impaired bone properties as they recovered and were “back to normal” at 3-6 months. However, 33% did not have their normal bone density at 1 year which makes one at an increased risk for getting another BSI. Stress fractures are typically given a grade. Higher grade stress fractures will take longer to heal. From a biomechanics standpoint, foot posture, strike pattern and cadence do not tell the whole story but can play a role. Studies show a 5-10% increase in step rate may be beneficial (7). This is where a PT skilled in treating runners comes into play. You will need guidance for a return to run program but that won’t be effective without drills that gradually add load (squatting, deadlifts, lunges). This can be a time to detect inefficiencies and compensations in your movement pattern with trained eyes on you.

INTERVENTION for Healthy Running
Early intervention is key to healthy running after bone stress injuries. Keep in mind that BSIs don’t warm up as you run like tendinopathies can. Bone stress reactions can lead to stress fractures but this isn’t inevitable if treatment is implemented early in the process. Endurance athletes should let their physicians know if they are feeling less motivation to run, are feeling run-down or feel like they take a long time to recover from an injury. There are some factors that we can be aware of that might contribute to a BSI. There is an increased risk in runners who run greater than 20 miles per week, people who run year-round and during a building phase of a running program. (8) Communication with your coach about how you are feeling is also essential so they can help you recover properly. This can help you avoid the feeling of yo-yoing between injuries. If you are increasing your training and not also increasing your intake of healthy food, your energy availability will be low.

Fueling on a run is key to success. Photo Credit Greg Spooner
Runners are used to digging deep so it can be hard to stop and reset when something feels not quite right. A registered dietician (RD) can be vital to recovery but also on the prevention side of things. Keep in mind that low energy availability does have a higher incidence in females due to its association with menstrual function and bone mass but remember it can also happen in males with overtraining or under-utilization of proper nutrition principles. According to Dr. Pritchett, “In our recent survey-based study using the LEAF-Q (Low Energy Availability in Female Athletes Questionnaire), we found that 53.04% of recreational runners (n=1923) were at risk for low energy availability”. She notes Team USA has nutrition guidelines for active individuals but each person should also seek an individualized plan that fits their needs. USOPC | Nutrition (9) From her Runner’s World article about ferritin levels, she notes “Ferritin is an important blood marker that is indicative of iron storage. There is a wide range for what is considered to be a ‘normal ferritin level’ ranging from 12-300 ng/mL. Runners tend to associate a poor performance with low iron. However, there are so many factors that influence performance, it is very difficult to link ferritin levels to performance. In fact, high iron levels can be toxic for the liver and heart. Therefore, acknowledging individual athlete standards, a ferritin level >35ng/ml along with normal hemoglobin is ideal.” (3)
““In our recent survey-based study using the LEAF-Q (Low Energy Availability in Female Athletes Questionnaire), we found that 53.04% of recreational runners (n=1923) were at risk for low energy availability.””
What is Bone Remodeling?
Ultimately, our body is working toward a state of homeostasis. Our bone is remodeling constantly through the use of osteoblasts (bone building) and osteoclasts (bone absorbing). When we are injured, that process starts immediately and its efficiency depends on the loads we put on these areas as they heal. That means we want to contract our muscles (ie exercise) as that signals a response for bone growth. (8) It should, however, be done in a guided manner to monitor the effects of gravity (which we need for bone health) and ground reaction forces (GRF) to be sure we don’t load too much too soon. Low energy availability can put runners at risk for injury and also slow their healing. Runners who keep cycling through one BSI after another are often in this camp, whether they realize the reason or not. If someone has LEA, the body will start to take calcium from the bone and this process sets people up for a BSI. Registered dieticians who work with runners will have a screening tool of questions that can get to the missing link and keep injuries from being recalcitrant in nature.
X-rays are often the first step in diagnostic imaging for BSIs. They can demonstrate many frank or overt stress fractures but not stress reactions or subtle stress fractures. (2) MRI or CT scan is the gold standard which often is combined with a DEXA scan to assess bone mineral density (BMD). It depends on which study you read, but ground reaction forces increase between 3-10x the body weight with running. Therefore, a gradual return to running program alone isn’t going to cut it after a BSI. Weight-bearing drills that gradually increase the load and eventually involve plyometric drills will better set someone up for tolerating the load of running. This will also help to keep a runner from getting another BSI. Physical therapists can work with running coaches to implement these movements into the daily routine. Running can use the muscles in a way that feels like you are constantly braking which is called eccentric loading. Therefore, we have to incorporate eccentric contractions into a complete running rehab routine. It is important to keep in mind that bone stress injuries were first identified in the military according to Dr. Adams. These were called march fractures from essentially doing too much too soon. This population tended to be healthy young males so they didn’t necessarily have the same issues facing some recreational and competitive runners today. These injuries tended to occur from just “taking it to the max” or pure volume overload. (2) This is why it’s important to look at the entire picture of an individual runner’s training plan.

HOw Does Bone Density Change with Age?
According to one study, runners don’t see the same rate of bone accrual from ages 13-17 as athletes in other sports (10). For young runners who run year-round, the risk of BSI creeps upward. So remember the benefit of including sports that require lateral movement into your routine and/or having an off-season where your running volume diminishes for a period of time. Disordered eating occurs in 6-45% of females and 19% of males according to another study (11). So don’t wait to seek the skills of a registered dietician if you suspect that of yourself or one of your athletes. This can also help to create lifelong habits of healing eating and body image.
““Running can be a way to explore the mountains, cool off after a busy day, clear the head and gain a general sense of well-being. Our goal as physical therapists is to identify an injury that might be presenting as a BSI so that we can modify the runner’s training plan as needed as well as get them to the proper member of the rehab care team.” ”
In conclusion, running can be a way to explore the mountains, cool off after a busy day, clear the head and gain a general sense of well-being (endorphins). Our goal as physical therapists is to identify early an injury that might be presenting as a BSI so that we can modify the runner’s training plan as needed as well as get them to the proper member of the rehab care team (MD, RD) and keep an open line of communication with coaches and parents to get an athlete back to running in a healthy manner. Each individual runner is different depending on their goals, training history and body type and I know I love being a part of a team surrounding an athlete that is determined to keep that in focus while concentrating on the end-goal of lifelong health.
On a side note, I know I found inspiration from a few notable runners who had injuries of their own. I highly recommend reading Good for a Girl: A Woman Running in a Man’s World by Lauren Fleshman, Out and Back: A Runner’s Story of Survival Against All Odds by Hillary Allen and Endure: Mind, Body and the Curious Elastic Limits of Human Performance by Alex Hutchinson. They don’t all have to do with BSIs but all touch on how the body responds after injury and are an interesting glance into the world of recovery even at the elite level.
AUTHOR:
Mandie Majerus, PT, MSPT, OCS, CSCS, SFMAc, CMPT, CFSC
CONTRIBUTORS:
Dr. Bob Adams, DO
ret. USATF Chair and ret. Primary Care Physician Evergreen Hospital
Dr. Kelly Pritchett
Professor Central Washington University
Ben Wobker, PT, MSPT, CSCS, CFSC, SFMA
Founder & CEO Lake Washington Physical Therapy
About the Author:
Mandie Majerus is a physical therapist at Lake Washington PT in Kirkland, WA. She is a co-founder of the Alpine Training Project as well as an avid backcountry skier and ski mountaineer. She grew up skiing, running and playing basketball in Bozeman, Montana and now enjoys every opportunity to ski in the N. Cascades of Washington State and the volcanoes of the west coast. Mandie works in the medical pool with the US Ski Team including covering World Cup races and camps as the on-site PT. She is a board-certified Orthopedic Specialist, Level I running coach, Certified Strength and Conditioning Specialist and Certified Manual Physical Therapist. She spent an austral summer season as the sole PT at McMurdo Station and the South Pole Station in Antarctica. Mandie is the manager of the downtown Kirkland location of Lake Washington Physical Therapy.
About the Contributors:
Dr. Bob Adams, DO is a sports medicine specialist in Kirkland, WA with over 45 years of experience in the medical field. He graduated from the University of Oklahoma for his undergraduate degree and served as a Naval officer through ROTC (Lieutenant) prior to going to medical school at Oklahoma State. He completed the first fellowship in primary care and sports medicine in the country. He served as the team physician for several area high schools as well as Seattle Pacific University and Seattle University. He was the chair of the USTAF Sports Medicine and Science Committee and was team physician for multiple World Championships and Olympic Teams. He served the USOPC as Team Physician and Doping Control Crew Chief and was Chair of USTAF Substance Abuse and Education Committee when they developed the first program for PED testing. He has lectured nationally and internationally and was most recently invited to the NCAA consensus meeting regarding their updated policy on Cannabis use. He was also past president and fellow of the American Osteopathic Academy of Sports Medicine and a fellow of the American College of Sports Medicine.
Dr. Kelly Pritchett is a Professor in Nutrition and Exercise Science at Central Washington University. As a board-certified specialist in sports dietetics, she has consulted with both elite and collegiate athletes as well as with active individuals. While in college, she competed on the swimming and diving team at the University of Alabama. Pritchett serves on the leadership committee of the Academy's Sports, Health and Performance Nutrition dietetic practice group as the Social Media Coordinator and served as a National Media Spokesperson for the Academy of Nutrition and Dietetics. Pritchett is an active member of the American College of Sports Medicine. She has authored research articles for scientific journals and presented at regional and national conferences. Her current research interests include post exercise nutrition for recovery, vitamin D and the athlete, and energy availability in athletes with spinal cord injury. In her spare time, she enjoys running and spending time with her three active boys.
MORE BLOGS





MORE WEBINARS
References:
1. Nathan Carlson, YouTube channel, How Do Stress Fractures Heal? - YouTube (with permission)
2. Dr. Bob Adams, personal communication, July 2023.
3. Dr. Kelly Pritchett, personal communication, July 2023.
4. De Souza MJ, et al. 2014 Female Athlete Triad Coalition Consensus Statement on Treatment and Return to Play of the Female Athlete Triad: 1st International Conference held in San Francisco, California, May 2012 and 2nd International Conference held in Indianapolis, Indiana, May 2013. Br J Sports Med. 2014 Feb;48(4):289. doi: 10.1136/bjsports-2013-093218. PMID: 24463911.
5. Papageorgiou, M., Dolan, E., Elliott-Sale, K.J. et al. Reduced energy availability: implications for bone health in physically active populations. Eur J Nutr 57, 847–859 (2018). https://doi.org/10.1007/s00394-017-1498-8
6. Popp KL, et al. Changes in Volumetric Bone Mineral Density Over 12 Months After a Tibial Bone Stress Injury Diagnosis: Implications for Return to Sports and Military Duty. Am J Sports Med. 2021 Jan;49(1):226-235. doi: 10.1177/0363546520971782. Epub 2020 Dec 1. PMID: 33259223.
7. Heiderscheit BC, et al. Effects of step rate manipulation on joint mechanics during running. Med Sci Sports Exerc. 2011 Feb;43(2):296-302. doi: 10.1249/MSS.0b013e3181ebedf4. PMID: 20581720; PMCID: PMC3022995.
8. Nathan Carlson, YouTube Channel, What Caused Your Stress Fracture??? - YouTube
9. Nutrition. Team USA website. https://www.teamusa.org/nutrition. Accessed July 30, 2023.
10. Nathan Carlson, Stress Fracture School, Continuing Education cohort Sept 2022.
11. Hart, N et al. Biological basis of bone strength: anatomy, physiology and measurement. J Musculoskelet Neuronal Interact 2020; 20(3):347-37